
 Podcast")
/
RSS Feed
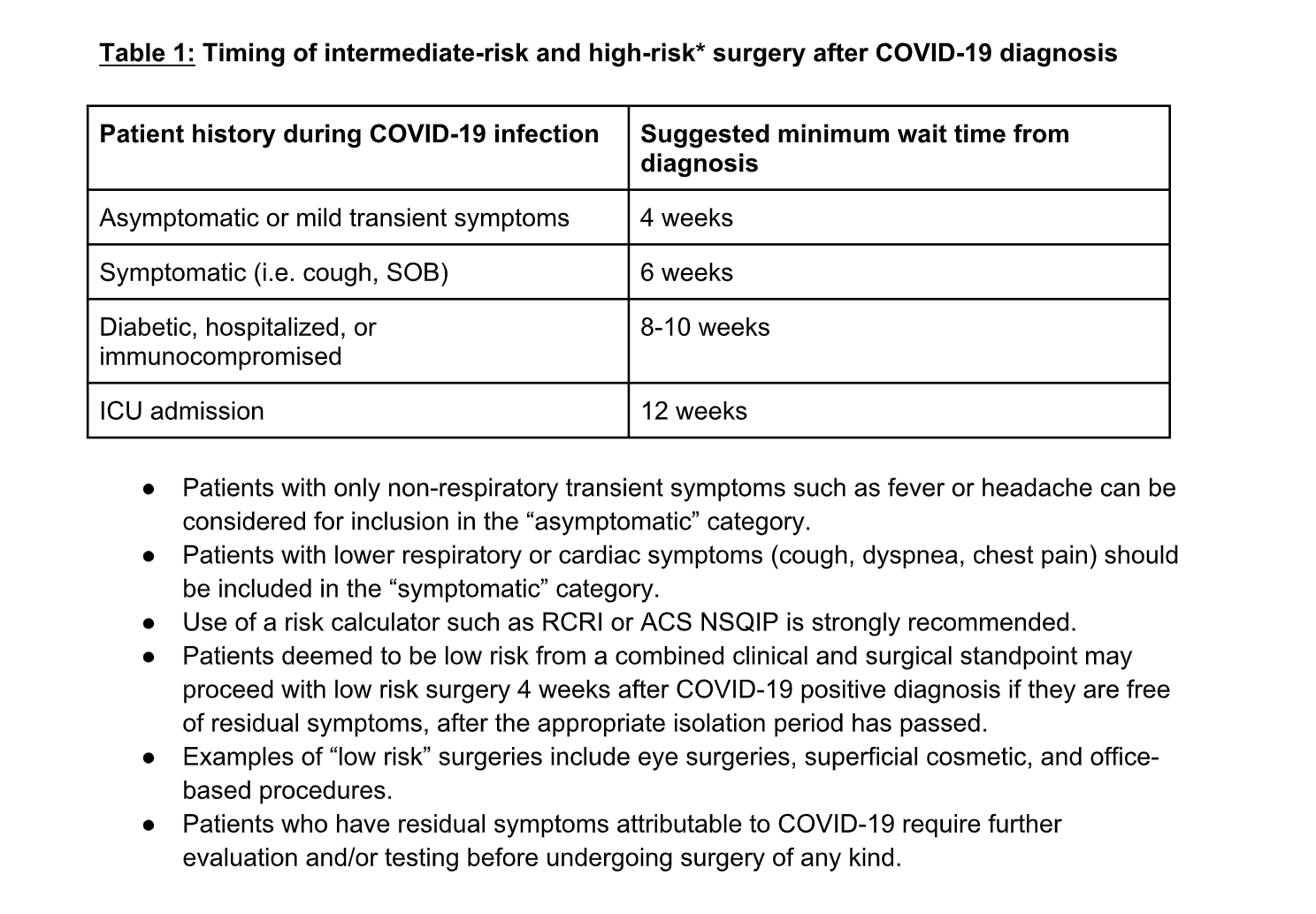
In this 189th episode I welcome Dr. Jason Chi to the show to discuss what we know about how to plan for surgery in patients who have recovered from COVID-19.
CME: https://earnc.me/3FlooY
Show Notes by Dr. Kashkooli
Jason’s email: ja**********@***il.com
{kind=link}
Random Recs:
Minari: https://youtu.be/KQ0gFidlro8
Doctors Without Borders: www.doctorswithoutborders.org
Daniel Tiger: https://pbskids.org/daniel/
Excellent podcast reviewing a potential approach to a clinical scenario we are going to see more and more!
Perhaps Dr. Chi can comment on whether the urgency/electiveness of a given procedure was a component of the algorithm. For example, were different waiting periods recommended for a patient wanting a total joint replacement, versus a patient needing myocardial revascularization?
Dr. Chi’s response is below:
We made a somewhat deliberate decision to leave out the urgency of the procedure as a consideration. There is very little evidence base which addresses the issue of urgency as it relates to post-Covid recovery and post-op complications. The closest thing we have is the CovidSurg collaborative of 122 patients who were all undergoing “curative elective cancer surgery”– according to the study data, the ratio for “early disease” versus “advanced/nodal disease” is approximately 60/40. Predictably, patients with advanced disease did more poorly, having a 6x higher risk of post-op pulmonary complications. However, the data set is very small and I am very hesitant to make recommendations based solely off of this study. This leaves us with very little else when evaluating the question of surgical urgency, post-Covid, and post-op complications.
My general approach is to consider our created timelines to be most applicable to elective cases (i.e. hernia repair, podiatry, total joints, etc.). For urgent cases, there is an elevated risk of complications which is inherent to the underlying reason for the urgency of the case (i.e. cancer, coronary disease–CABG). At this point we cannot tease out how much of that elevated risk comes from a recent covid infection versus the underlying disease process. In these cases I inform both the surgeon and patient that there is an increased risk of post-op complications, particularly in those who were symptomatic from Covid and/or have pre-existing pulmonary disease, and that this increased risk is currently poorly quantified. As generic and unsatisfying as it sounds, a risk-benefit discussion should then determine when and how to proceed.
Hope this helps, and feel free to contact me with any other questions!
Thank you. This was excellent and I’m sure something that we will continue to explore in the future. Just like the post-polio patients from the 1950s, we probably will be dealing with the long-term ramifications of SARS-Cov-2 infection for some time.
I would love to hear a follow-up with Dr. Chi. It also would be interesting to do an episode dedicated to his time volunteering with MSF.